The medical device was designed for Electrophysiologists. That was the problem.
How recentering a Class III medical device around its true primary user — the Pacer Nurse — transformed St. Jude Medical’s market position and produced a product the industry lauded for years.
CLIENT: St. Jude Medical Cardiac Rhythm Management Division (now Abbott)
INDUSTRY: Cardiac Rhythm Management / Class III Implantable Devices
SERVICES: Ethnographic Research · Persona Development · Interaction Design · Human Factors Engineering · Usability Testing · Design Leadership
A RELATIONSHIP BUILT ON RESULTS
St. Jude Medical is a part of Lizz Bacon’s career spanning nearly seven years and three distinct chapters — and it begins with a cold start. I first engaged with St. Jude Medical as a consultant; then I was brought on full-time because of what the early work demonstrated and subsequently spent almost five years building the human factors design function from the inside. Then after I founded Devise, I was engaged as a consultant again for another year and a half: St. Jude was, in fact, Devise Consulting’s very first client.
| 1 | Consultant | Initial engagement — 4 months. Field research and persona development, Interaction Design framework laying the groundwork for the Merlin PCS solution. |
| 2 | In-house | Joined full-time as Senior Human Factors Design Engineer — nearly 5 years. Led the entire software design and user validation efforts, supporting market launch and subsequent iterations of the Merlin PCS platform. Led the research, design and market launch of the Pacing System Analyzer. Grew the design team from 1 to 6. |
| 3 | Devise Consultant | Devise’s first-ever client — 1.5 years. Continued to provide design, requirements, and human factors engineering support for evolutions of pacemaker and ICD products, drawing on deep institutional knowledge. |
This arc — from consultant to employee to consultant again — tells its own tale, speaking to the kind of trust that only comes from consistently delivering in a high-stakes environment over a sustained period. My time at St. Jude also shaped how I think about client relationships: the best are long-term, built on genuine mutual respect for what each side brings.
THE SITUATION
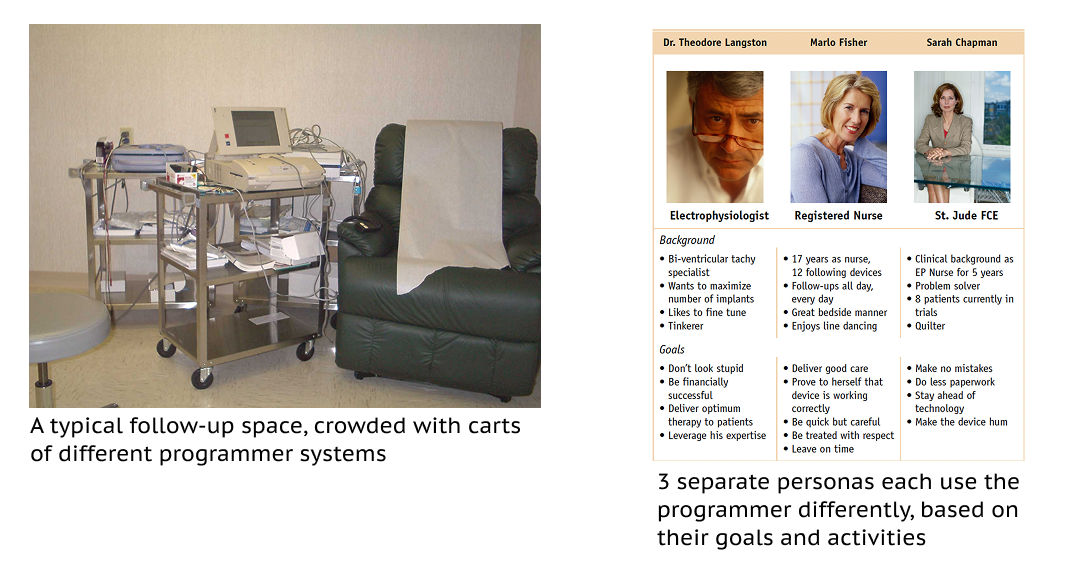
The Merlin Patient Care System (PCS) Programmer is a hardware and software system used to monitor and update Class III implantable cardiac rhythm management devices — pacemakers and defibrillators. It’s used in cardiology clinics across the country, typically in dedicated “follow-up” rooms where patients come in to have their implanted devices checked and adjusted. The stakes are about as high as they get in medical technology: the devices being managed are keeping people’s hearts beating properly, or restoring the heart to beating with an electrical shock after cardiac arrest.
As the first Senior Human Factors Design Engineer at this Fortune 100 company — a role I helped define and then helped build into a six-person team over five years — I led the user research, interaction design and requirements definition, as well as user validation efforts that would drive the entire Merlin PCS product direction.
THE INSIGHT THAT CHANGED EVERYTHING
The existing system had been designed with the Electrophysiologist in mind — the physician at the top of the cardiac hierarchy, with an advanced and highly technical understanding of the heart as an electrical system and a specialized clinical vocabulary to match. That’s a reasonable-sounding design target. It was also wrong.
After extensive field research at clinics across the country — observing how the Programmer was actually used, by whom, and in what context — the picture became clear. The person using this system day in and day out wasn’t the Electrophysiologist. It was the Pacer Nurse. And a software system designed for an EP with their highly-specialized vocabulary was, unfortunately, a system which was genuinely hard for a Pacer Nurse to use.
Lizz realized: The nurse is the key role driving the “follow-up” clinical workflow — and she has been designed out of her own primary tool.
This pattern unfortunately repeats throughout healthcare technology: systems get designed around the most technically sophisticated user in the room, while the most frequent and operationally critical user is someone else entirely. Getting your primary user profile wrong doesn’t just create friction — in a Class III device context, it creates risk. Nurses could be missing critical bits of information and important device tests because the features were presented in obscure ways.
THE APPROACH
The original field research spanned clinics all over the country and was ethnographic in approach — meaning we were there to observe and understand, not just interview. We watched Pacer Nurses move through their actual workflows: how they set up the room, how they ran a follow-up session, what they needed to know first, what they had to navigate around, where the cognitive load was highest.
From that research, we built a full persona set representing the cast of people who interact with the Programmer system. The primary persona — Marlo Fisher, the Pacer Nurse — became a genuine organizational touchstone. When we understood her mental model, we could design everything around that insight and make the whole system more usable.
NOTE: A key factor to consider in this St. Jude Medical case study is what good product research, design, and innovation looks like in a highly regulated environment. As a manufacturer and distributor of Class III medical devices, we faced significant compliance obligations to follow both American and International regulatory guidance (including the ANSI/AAMI HE75:2009 and IEC 60601-1 regulatory frameworks). The happy news is that following a thorough user-centered research and design process is strongly compliant with both FDA and IEC regulations. If you’re interested in this topic, please read more about this angle in the whitepaper Interaction Design for Medical Systems.
THE DESIGN
This battery check was followed by a rapid sequence of checks testing the proper functioning of the device. Only occasionally was device re-programming involved, typically performed by the physician.
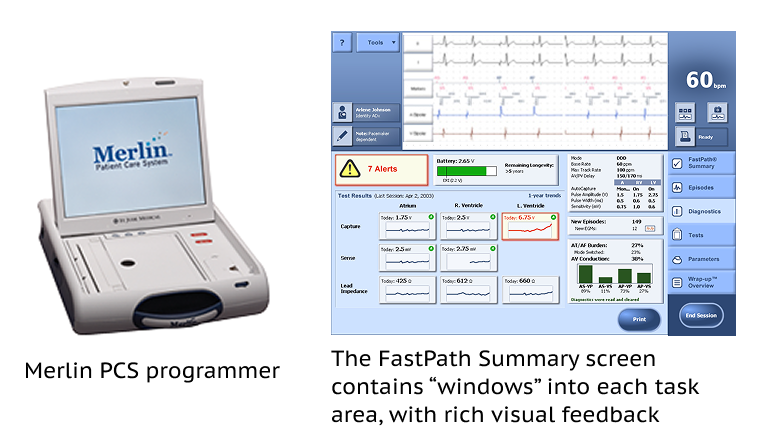
The centerpiece of the Merlin PCS redesign was what became the trademarked FastPath Summary screen — a single top-level view that consolidated every basic check Marlo performed into one place, with the battery longevity positioned prominently at the top. Marlo’s first priority was supporting the patient with their top question about device longevity: how long until they need a replacement procedure? The battery longevity display — the element at the top of the FastPath Summary that tells Marlo, at a glance, how long before the patient’s device needs replacing — is something I’m named on a patent for. It’s a small thing in isolation. In the context of a Pacer Nurse managing a full clinic of patients with implanted devices, it’s the first question answered in every single appointment.
Each visual panel on the screen offered what I called a “window into the room”: a meaningful summary of the full set of operations and data behind it, giving Marlo instant orientation while keeping the depth of detail accessible when needed. The logic we made legible behind the standard follow-up workflow became the information architecture of the redesigned software.
Another key insight was creating a dedicated final screen: the “Wrap-up Overview” became a trademarked feature of the Merlin PCS solution. This architecture accomplished something that sounds simple but is genuinely difficult to achieve: it made the system fast and intuitive for the Nurse without removing any of the technical power and detail that the Electrophysiologist and/or Cardiologist required. Designed for Marlo, it worked beautifully for everyone.
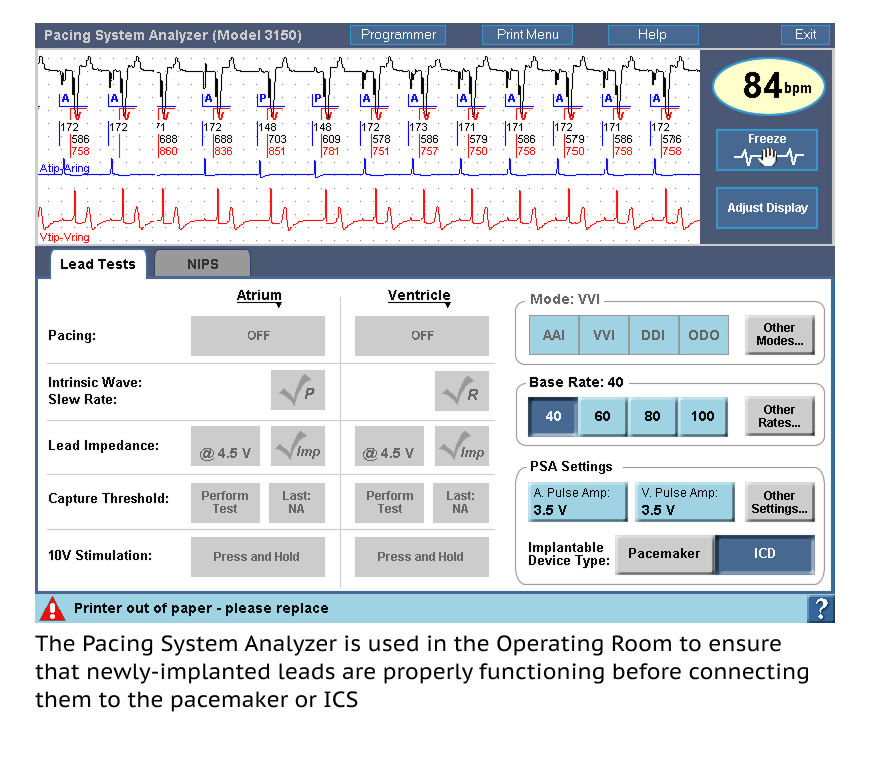
In addition to the Merlin PCA, I led the human factors research, design, and user validation of a new Pacing System Analyzer solution for St. Jude Medical. This project involved observation of actual device implant procedures in the operating room, and also informed industrial design decisions in concert with the software definition.
Understanding the physical constraints of the OR context (sterile fields, clinical distance requirements, the pace and pressure of a live procedure) shaped things like cabling length and the imperative of rapid, automated device testing.
THE OUTCOME
Closing in on market leadership
After the Merlin PCS launched, St. Jude Medical moved rapidly from a distant third in the cardiac rhythm management market to a close second behind Medtronic — a significant commercial shift directly linked to the product’s reception.
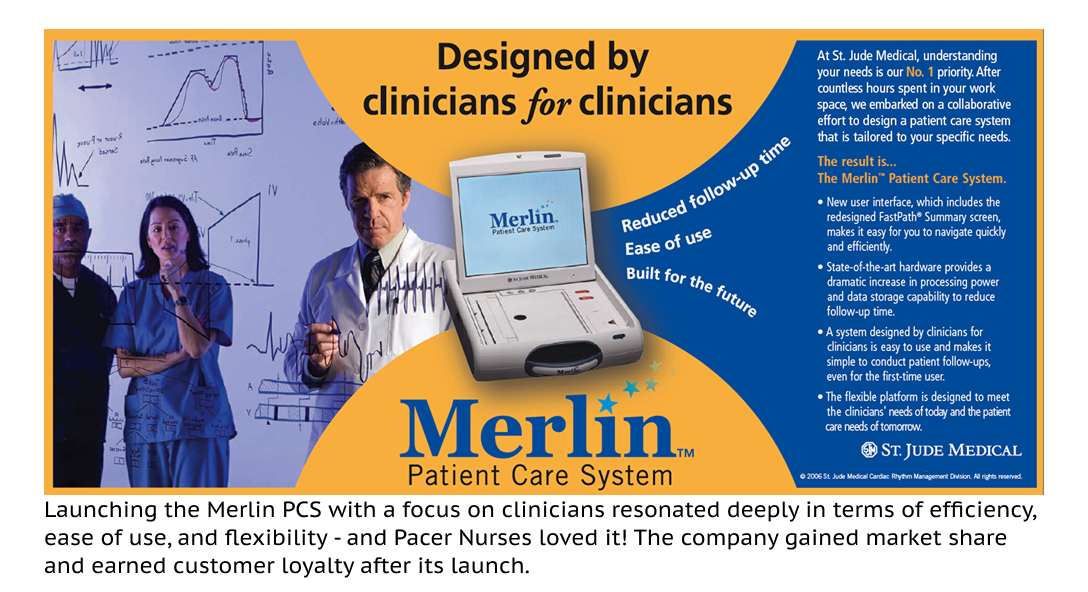
“Designed by clinicians, for clinicians”
The product’s marketing tagline captured what the field research had made possible. Pacer Nurses in particular responded to the product with genuine enthusiasm — a rare outcome in a market known for tolerating difficult tools.
A named patent and a lasting design
The FastPath Summary’s battery longevity display resulted in a named patent — and the overall design process and approach informed St. Jude’s product development culture for years afterward.
This engagement shaped how I approach one of the most fundamental questions in healthcare UX: who is our real primary user? In complex clinical environments, the answer is often not who you’d first assume. While the physician is often the most visible actor in the room, frequently it’s the nurse, the technician, or the care coordinator whose workflow the system has to serve, day after day, to function safely and efficiently. Achieving that clarity isn’t just good UX practice: it supports the business’s bottom line because better usability in a healthcare context leads to improved adoption and retention.